
Membership Groups
The Union's scientific sections and working groups offer members an opportunity to work with others who share the same interests and collaborate on research, publications and projects. They propose sessions and contribute to the planning of the Union World Conference on Lung Health, and influence the future of lung heath through the governance of The Union.
The Union is divided into seven regions to provide a platform for addressing lung health and related issues from a regional perspective, allowing members to network with colleagues who face the same challenges and contribute to The Union's deep understanding of local issues.
Working Groups
The Union's working groups offer members an opportunity to affiliate with others who share the same interests and collaborate on research, publications and projects.
If you are interested in these issues, become a member of The Union, and then you are welcome to join whichever working groups you like.
Members may also propose and manage their own working groups.
ADULT AND CHILD LUNG HEALTH
The Post Tuberculosis Lung Disorders Working Group conducts research, investigates strategies and raises awareness amongst healthcare workers and policy makers on post TB lung health.
Goal: To serve as a community of practice for investigators, program managers, and advocacy groups who are working to improve TB prevention, detection, and treatment for women and children by integrating TB and TB/HIV services in maternal and child health settings
Objective: To share information about promising practices and experiences with country implementation; disseminate informational, educational, and communications resources; advocate for increased attention to the needs of women and their children with TB and TB/HIV; and close critical research and practice gaps in this field
Current Activities:
- Continued advocacy around inclusion of Maternal TB notifications in the Global TB Report
- Advocacy including raising awareness about maternal/infant TB among TB and non-TB-focused fora and conferences
- Advocating for maternal/infant variables in the drug-resistant TB individual patient database
- Continue working on Cochrane Review TB Symptom Screen in Pregnancy
- Hosted a meeting to develop a TB and Pregnancy Guide
Recent Maternal and Child Tuberculosis achievements:
Inclusion of Maternal TB Notifications in the Global TB Report. We sent a detailed motivation to the WHO GTB. Their response was generally favorable, but WHO GTB concerns about workload for individual countries and the lack of electronic based systems in many high-burden countries.
We surveyed 5 countries with case-based electronic systems for their ability and desire to collect data around maternal TB. Four of five countries (Brazil, Lesotho, South Africa and Zimbabwe) responded to the survey. All four countries agree with the importance of collecting these data. However, in 3 of 4 countries, current systems would not allow easy collection and reporting of these data at this time, though they did indicate a desire to update their systems.
STAG: We continued to advocate for a maternal TB representative appointed to the Strategic and Technical Advisory Group for Tuberculosis (STAG-TB).
Research
Continued Work on a Pregnancy Registry: The US FDA attempted to establish a CURE Drug Repurposing Collaboratory (CDRC) to make a “Pregnancy Treatment Repository” publicly available. Due to insurmountable logistical challenges, this is no longer being pursued. The DR-TB individual patient dataset (IPD) is now being hosted at and curated by UCL, in collaboration with WHO GTB. We are exploring opportunities to add pregnancy and infant variables as well as how to link maternal and infant data. Initial discussions were favourable.
Advocacy
- Raising awareness among TB and non-TB-focused conferences
- Pregnancy, HIV, and Tuberculosis: Current Practices and Research Opportunities
- US National TB Controller Conference: Tuberculosis in Pregnancy
- TB and Pregnancy Guide: A group was established and partners were chosen. We aim to develop a collaboration of researchers, clinicians, patients and advocates to develop a Tuberculosis in Pregnancy Field Guide. This field guide will share evidence and best practices for preventing, diagnosing and treating DS and DR-TB among pregnant and postpartum women and their infants with a focus on low-resource settings. Advocated for a Maternal & Neonatal TB Representative in the core team of the child and adolescent TB working group (hosted by the Stop TB Partnership).
This working group focuses on chronic respiratory problems, across the life course with the goal of advocating for challenge-focused research that is inclusive, equitable and strengthens links between researchers, communities and policymakers.
Completed activities/ contributions/publications:
· GOLD International COLD Conference, United Kingdom & Africa Satellite Program
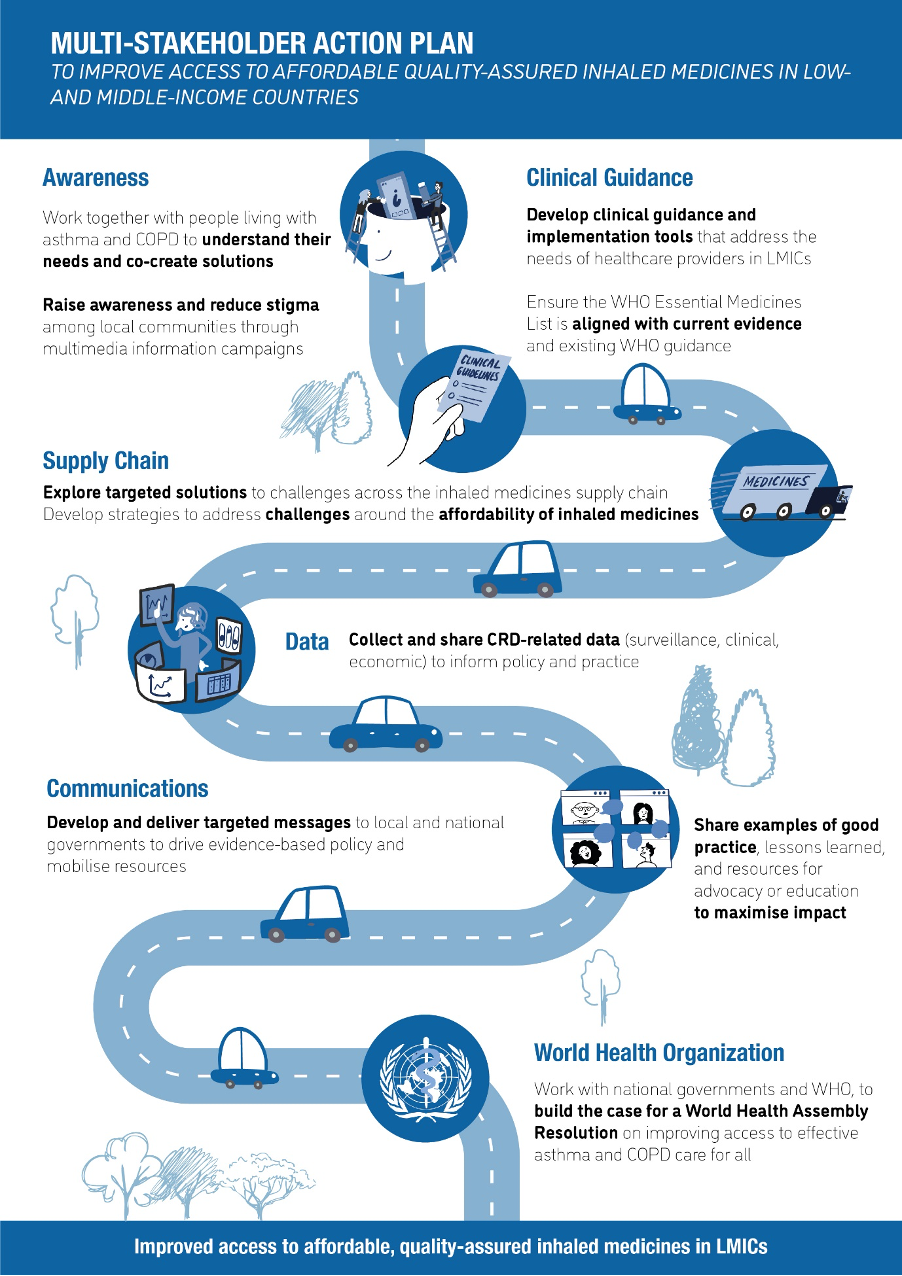
· Multi-action virtual stakeholder meeting: Action Plan Formulation, The Union hosted.
Improving access to affordable quality-assured inhaled medicines in low- and middle- income countries. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4107776
· Patients with presumed tuberculosis in sub-Saharan Africa that are not diagnosed with tuberculosis: a systematic review and meta-analysis.
Future activities:
· Qualitative study: Barriers and facilitators to implementation and uptake of inhaled medicines for the treatment of chronic respiratory symptoms in The Gambia. Data collection in progress. Formulation of future patient and public engagement group.
· Coordination of IJTLD ‘Clinical Standards on asthma management in Low/Middle Income Countries’ Delphi process.
· Patients with presumed tuberculosis not diagnosed as tuberculosis: a global systematic review and meta-analysis. PROSPERO CRD42022301016. In progress
· Systematic review - Prevalence of bronchiectasis in Africa In progress
· Kenyan Medical Research Institute – Non communicable disease in Kenya: Burden, early life determinants and interdisciplinary participatory solutions. Data analysis ongoing
· Burden of Obstructive Lung Disease (BOLD) in Nairobi and its neighbouring counties. In progress
CHILDHOOD PNEUMONIA WORKING GROUP
Adult and Childhood Lung Health Scientific Section, The Union
Authors: Eric McCollum, Rebecca Nantanda, Leith Greenslade
Overall Goal
To establish a child pneumonia hub within the Union to:
- Amplify evidence and policy solutions with the capacity to accelerate reductions in child pneumonia deaths
- Strengthen community of practice across child pneumonia researchers and advocates linked to The Union and beyond
- Influence the global agenda on child pneumonia through high visibility convenings and presentations at major global health events, including the annual Union World Conference on Lung Health
Given the concentration of child pneumonia deaths in low- and middle-income countries (LMICs), the group is committed to supporting scientists, research institutions, and implementation research based in these countries.
Background
Each year pneumonia kills more children less than five years of age than any other infectious disease, according to the Global Burden of Disease The most recent data estimate that 610,000 children died from pneumonia in 2023 . Almost all of these deaths occur in low-and middle-income countries (LMICs) and three in every four are in the Sub-Saharan African (307,000) and South Asian (160,000) regions.
Although child pneumonia mortality has fallen by 56% since 2000, these reductions have lagged other leading causes of child death, including diarrhea (-72%), measles (-80%), meningitis (-63%), and tuberculosis (-59%) (2). To achieve the child survival Sustainable Development Goal (SDG) by 2030, child pneumonia deaths need to fall to below 400,000.
This target is achievable using existing prevention, diagnosis, and treatment tools, many of which are under-implemented in high burden settings. Key interventions include:
- Vaccines targeting the leading causes of pneumonia, including pneumococcus and respiratory syncytial virus (RS
- Improved diagnostic tools, including emerging AI-enabled technologies
- Medical oxygen systems and pulse oximetry
- Child appropriate antibiotic formulations
- Nutrition interventions targeting severe malnutrition –the key pneumonia mortality risk factor– including breastfeeding, small quantity lipid-based nutrient supplements (SQ-LNS), and treatment of wasting using ready-to-use therapeutic food (RUTF)
Aligned with the Prevent, Protect and Treat (PPT) framework for pneumonia control, additional priorities include:
HIV prevention and treatment
Reducing household air pollution, especially exposure to second-hand tobacco smoke and biomass fuel emissions
If governments act decisively to ensure that every child can access this full package of proven interventions—vaccination, early diagnosis, medical oxygen, appropriate antibiotics, and nutrition support—pneumonia would be transformed from the leading infectious killer of children and countries would make rapid progress to achieving the child survival SDG.
The Union’s expertise and longstanding activism to highlight tuberculosis and other lung diseases pertinent to LMICs, positions the organization to elevate child pneumonia on national, regional, and global health agendas. The Union has yet to incorporate child pneumonia as an area of focus despite its clear mandate to lead on child lung health. The working group will support The Union to address this, serving as a multi-disciplinary child pneumonia hub for researchers, policy makers, implementation partners, healthcare providers, and donors
Members
The group seeks to engage leading and emerging child pneumonia researchers, especially those based in LMICs. In addition, government officials, global health agencies, NGOs and civil society, and professional societies are all welcome.
Members will benefit from:
- Quarterly meetings, including at least one in-person convening
- A regular email newsletter highlighting the latest peer-reviewed research, conferences, funding opportunities, and more
- Access to a global directory of child pneumonia researchers
- Opportunities to present in child pneumonia sessions during major global health conferences
- Participation in an annual World Pneumonia Day webinar (12 November)
Member activities will be highlighted through the newsletter, website, and social media channels.
Join the Working Group
Union members can select groups in their membership account here or get in touch on membership@theunion.org
For more information, contact:
Eric McCollum - emccoll3@jhmi.edu
Leith Greenslade - leith@justactions.org
Overall Goal:
To improve child health globally by advocating for - and contributing to - clinical research, implementation science, and providing an evidence base for policy-making that addresses the challenge of co-occurring TB and severe acute malnutrition (SAM) in children.
Group Objectives:
Improve awareness in the global child health community of the strong association between TB and SAM, and the need for focused intervention and development of models of care for these two conditions.
Promote, and advocate for, research to improve the understanding of key areas for management of TB and SAM: epidemiology; screening, diagnosis, and prevention of each condition in the face of the other; and optimized treatment of TB for children with SAM.
Promote evidence-based policy-making that addresses the burden of co-occurring TB and SAM in children.
Working Group goal:
To develop and promote a strategic policy agenda on quality improvement package for the diagnosis, treatment and management of asthma
Background:
With a mandate to bridge the gap between the scientific disciplines related to tuberculosis (TB) and lung health; the Union adapted the TB model for the management of Asthma, and worked with partners to implement comprehensive lung health project funded by the World Bank.
The idea of The Union’s Comprehensive Approach to Lung Health, was the adaptation of the TB model and apply the DOTS principles for the management of patients with chronic airflow limitations”. Pilot projects in Benin, China, El Salvador and Sudan generated valuable lessons on implementing standard case management for asthma and reducing the cost of medicines as a barrier to asthma treatment in resource limited settings.
It is a comprehensive package where The Union designed ADF and provided countries with procurement and quality assurance services, as well as technical support related to selecting, quantifying, managing and using essential asthma medicines. These services were accompanied by The Union’s technical guidance about how to establish asthma programmes in the general health services and generate data for quality improvement and policy advocacy. The technical guidance included tools (The Union’s asthma guidelines to diagnose and treat asthma with a combination of inhaled bronchodilators and corticosteroids, training materials and information system) and assistance with programme evaluation’ quarterly reports.
Objectives:
The objectives of the working group are to:
1.Sustain a platform of discourse and exchange of experiences and propositions among members regarding the management of Asthma.
2.Conduct an online survey on “Asthma Management Situation” for countries interested in The Union Model and write a report/publish the survey results.
3.Assemble and deliver special sessions on Asthma management at the Union World Conference on Lung Health in 2024/27.
4.Review the Asthma training Materials and The Union Asthma Guideline.
5.Develop a course for young Union consultants on Asthma management related to the Union Model.
6.Conduct a multi-country pilot/ revive the existing in-country experiences
7.Fund raising: explore the feasibility of using the member states call for integrating the prevention and control of non-communicable diseases in HIV/AIDS, tuberculosis, and sexual and reproductive health programmes.
TOBACCO CONTROL
The MPOWER Research Group on Tobacco Control was formed in the year 2017 with a goal to scale-up global tobacco control research for feeding into policies at regional/country level. The group was set up with the felt need of systematically mapping, identifying and prioritizing research (in terms of national priority) needed to implement the WHO Framework Convention on Tobacco Control and MPOWER in LMICs. The group is working on identifying key gaps and challenges in research focusing upon emergence of newer tobacco and nicotine products; tobacco industry interference; smokeless tobacco products; tobacco free generation; undertaking inter-disciplinary, multi-country research; integration of tobacco control with various programs and policies; and write position papers to address the attention of policy makers for marching towards a tobacco free future.
Recent MPOWER achievements:
The working group has generated 7 case studies on industry interference in different domains of tobacco control policy implementation in India.(viewable HERE)
Second, working group has published a position paper in the Indian Journal of Tuberculosis on ‘Fuelling the tuberculosis epidemic: The role of tobacco control in ending the TB emergency’.
A Special issue on Tobacco Control was published in Indian Journal of Tuberculosis (IJT) in 2021 that had a collection of manuscripts covering wide range of topics pertaining to tobacco control. (viewable HERE)
A supplement issue covering the proceedings & scientific abstracts from the National Conference on Tobacco or Health, held in 2021 in India was published in the Indian Journal of Cancer
Pilot projects on tobacco cessation are being implemented in community settings and hospital settings to strengthen the ‘O’ component of MPOWER.
TUBERCULOSIS
The TB and Migration working group focuses on tuberculosis among migrants, including epidemiology and risk factors in countries of origin, during transit and after arrival in countries of destination, and during their potential return. The group supports this emerging and under researched field through webinars, symposia, conferences and scientific papers and has a role in informing policy within The Union.
Work includes webinars, symposia, and advocacy - including influencing policy (e.g. drafting statements etc).
Recent TB and Migration achievements:
- A significant presence in Union conferences, including another symposium this year on TB and forced migration
- A TB and Migration website
The TB Infection Control working group is focused on the monitoring and evaluation of tuberculosis infection controls in health facilities and health systems.
The Global Indigenous Stop TB Initiative (GISI) Working Group of The Union has operated for over 15 years as a networking space for researchers, care practitioners, and advocates, to network and share our activities globally. To achieve our objective of increasing Indigenous Peoples’ involvement in and control over TB policy and programming, we began learning from the International Indigenous HIV & AIDS Community (IIHAC; https://iihac.org/). IIHAC is an Indigenous-owned organization incubated through Communities Alliances and Networks (CAAN; https://caan.ca/). In the last 4 years, GISI has been working with Trevor Stratton, a leader in CAAN and IIHAC, to learn about IIHAC’s history, development, and work and how they might inform GISI’s work in TB among Indigenous Peoples globally.
Achievements
To this end, an informal understanding started developing between CAAN and GISI, with a Venn diagram drawn to delineate areas of respective responsibility. Rather than attempt to make a formal Memorandum of Understanding (MoU) between the organizations, an Indigenous version on an MoU was proposed by Trevor Stratton, whereby the Chair of GISI, Dr. C. Andrew Basham, was invited to attend the 9th International Indigenous Pre-Conference on HIV & AIDS on July 26-28th, held in Montreal, Canada, preceding AIDS 2022 (the International AIDS Society’s main conference), July 29th-August 2nd 2022, also in Montreal.
On July 29th, 2022, a blanket ceremony was held between CAAN and GISI to develop an understanding of each other and create a relationship. This ceremony followed Indigenous protocols for gift-giving and story sharing to form an understanding of each other. In this ceremony, members of GISI and CAAN spoke about their backgrounds, their work, and their hopes for the relationship being formed. Dr. Basham was presented with a buffalo blanket and medicine bundle, after offering tobacco to CAAN Knowledge Keepers, along with two Harvard University mugs (representing something from his world). After receiving the blanket, Andrew made a short speech about finding and sharing the truth together to improve TB prevention, diagnosis, and care with Indigenous Peoples. This ceremony was concluded with a traditional song after a teaching by Dr. Albert McCleod, Elder-in-Residence at CAAN, who has been an HIV/AIDS activist since 1987.
CAAN held a webinar on March 31, 2022 about the lived experiences of Indigenous Peoples affected by TB in Canada that was moderated by Trevor Stratton and is available here and includes some discussion of the developing relationship between CAAN and GISI as well: https://www.youtube.com/watch?v=UWSyeHhu4yg
 Buffalo Blanket Ceremony: Communities, Alliances, and Networks (CAAN) with Global Indigenous Stop TB Initiative
Buffalo Blanket Ceremony: Communities, Alliances, and Networks (CAAN) with Global Indigenous Stop TB Initiative
(L-R: Trevor Stratton, C. Andrew Basham, Margaret Kisikaw-Piyesis. Photo by Stephen John)
The goal of the TB and Mental Health working group is to establish a community of practitioners and researchers to advance attention to mental illnesses and substance abuse in the context of tuberculosis care and control. Mental illnesses, such as depression and PTSD, and substance use disorders, such as alcohol and opioid dependence, are strongly associated with tuberculosis; populations affected by mental health disorders are typically vulnerable and at higher risk for tuberculosis infection, and individuals with tuberculosis often suffer from these disorders, complicating and undermining care and resulting in poor treatment outcomes. Nevertheless, formal attention to mental health is lacking in most tuberculosis control programs.
The Drug Resistant Tuberculosis working group goal is to gather and share information to help accelerate scale-up of evidence-based DR-TB policy and practice.
The working group surveys members at regular intervals to get a good picture of how MDR-TB treatment rollout is progressing in the various regions. In addition, the group has recently been focusing on the availability of susceptibility testing for the new and repurposed second-ling drugs. In addition, the group in collaboration with RESIST-TB, provides webinars and a newsletter focusing on new developments and publications on DR-TB.
Recent Drug-Resistant TB group achievements:
An article describing the results of our most recent survey “Global availability of susceptibility testing for second-line anti-tuberculosis agents” is in press in the IJTLD. Plans to link with rGLC through webinars, compilation of Key PMDTs related materials and dissemination
The TB and Ethics working group aims to encourage broader engagement with ethical issues in tuberculosis research and practice. The group promotes reflective and practical consideration of ethical issues within the TB community, particularly through Union conferences, development of educational case studies and other materials and peer-reviewed publication.
This working group was formed to set up a community of practice in tuberculosis multimorbidity, aiming to develop and promote a strategic research, awareness, advocacy and policy agenda and initiatives on physical and mental multimorbidity in tuberculosis care.
TB-Multimorbidity (TBMM) Working Group was formed to set up a community of practice in tuberculosis-multimorbidity aiming to develop and promote strategic research, awareness, advocacy and policy agenda and initiatives on physical and mental multimorbidity in Tuberculosis care. TB-MM Working Group will assemble researchers, practitioners and professionals to collaboratively focus on the advancement of implementation and operational research and practice, pertinent to addressing multimorbidity in tuberculosis. People diagnosed/cured with tuberculosis and comorbid conditions and their caretakers, being the most significant stakeholders, will also be included in the community of practice.
The objectives of this working group are:
1. To create and sustain a platform to pursue improvement in prevention, recognition and management of multimorbid physical and mental conditions in TB, through discourse and exchange of ideas, experiences and proposals, promotion of awareness and dissemination of the best practices and evidence.
2. To support and enhance the scope of collaborative research in TB multimorbidity through the formulation of an international research team and development of demonstration research project proposal/s for intervention/s for timely recognition and management of coexistent Non-Communicable Diseases in TB services and identification of pertinent funding sources.
3. To enhance the research capacity of early and middle career researchers in the area of TB multimorbidity to support them as potential research leaders, and to contribute to the operational research training initiative of the Union.
The key members of the group are Professor Kamran Siddiqi (University of York, UK), Dr Lloyd Friedman (Yale University School of Medicine USA) and Dr Alexander Jarde (Cochrane, France) in addition to many esteemed UNION members of this group.
The TB Undernutrition working group was established to highlight the importance of undernutrition as a risk factor for TB disease by engaging key stakeholders, providing critical analysis of bottlenecks to addressing this modifiable risk factor, and by helping identify innovative, strategic, and tailored responses to the delivery and scale-up of collaborative TB/undernutrition activities.
According to the Global Tuberculosis report 2021, Undernutrition is the leading risk factor for TB with a population attributable fraction of 19% which is higher than human-immunodeficiency virus (7.6%) and diabetes (3.1%). Being undernourished is associated with unfavorable treatment outcomes and mortality. Lastly, undernutrition is comorbid with other key TB risk factors including HIV and alcohol use and has implications for sustainable development goal 2 (zero hunger) and is, as such, a cross-cutting issue.
To propel action on nutrition in the context of TB, the working group plans to do the following:
- Highlight importance of nutrition in the TB pandemic
- Identify knowledge gaps, research priorities, and advocacy tools
- Develop content on undernutrition-TB for the Union’s website
- Engage stakeholders
- Organize two annual webinars
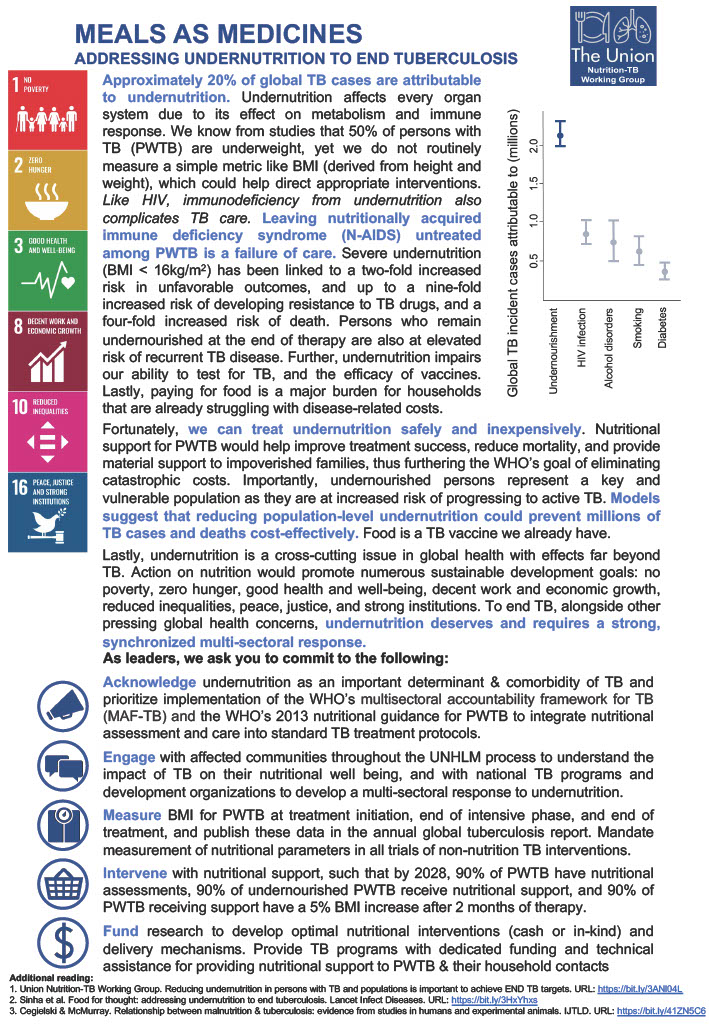
(Click to enlarge the above report)



Globally, people deprived of liberty (PDL) have extremely high rates of tuberculosis, often more than 10 times greater than the general population.1,2 Overcrowding, poor ventilation, limited access to healthcare resources, substance abuse and undernutrition are all risk factors that disproportionately affect PDL.3–6 At the same time, this population remains frequently neglected by Ministries of Health and Justice and in global TB prevention and care strategies. There is a critical need to increase attention and resources towards addressing the crisis of tuberculosis among PDL.7
The TB in Prisons Working Group seeks to engage practitioners, researchers, policy makers and advocates in raising awareness about tuberculosis among PDL and identifying and sharing best practices and guidance to improve care and prevention of TB in prisons. The Working Group will engage Union members in structured interactions to share experience and expertise on tuberculosis in prisons, to identify knowledge gaps and key areas for research, to build collaborations and consortia for research and implementation, and to create literature including reviews, perspectives, best practices documents and implementation guidance for areas where WHO guidelines are lacking. A major overarching goal of this Working Group will be to build a community of researchers and practitioners engaged in TB care and prevention in prisons to facilitate knowledge exchange and organize more effective, collaborative research and advocacy.
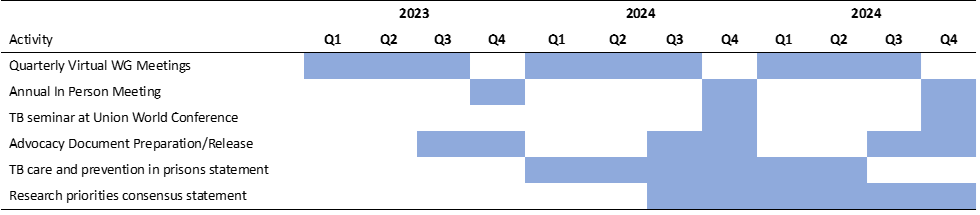
Objectives, by year:
2023: Hold a series of virtual meetings with rotating presenters on key themes in tuberculosis in prisons; hold in person meeting at Union World TB Conference
2024: Produce and distribute advocacy materials; continue regular virtual Working Group meetings; hold TB seminar and in person meeting at Union World TB conference;
2025: Finalize and distribute consensus statements on research priorities and TB care and prevention approaches in prisons; hold TB seminar and in person meeting at Union World TB conference
Activities:
We will invite working group members to participate in activities, including giving presentations virtually and at Union meetings, writing or providing feedback on advocacy documents, fact sheets and consensus statements, and participating in meetings with stakeholders. We will also seek to engage practitioners, clinicians, researchers and implementers who are not currently part of the Union to join the Union and play a role in the Working Group.
End deliverables:
- December, 2023 – Hold at least three virtual meetings and an in person meeting at Union World Conference to shape detailed agenda for the Working Group
- March, 2024 - Complete fact sheet and advocacy materials, distribute on World TB Day
- December, 2024 – Seminar and annual meeting at Union World Conference; Release advocacy strategy and updated materials
- December, 2025 – Release consensus paper on research priorities; consensus paper on TB care and prevention in prisons; Seminar and annual meeting at Union World Conference
Time frame & proposed date of completion:
Gender is one of the most important social determinants of health and should be a critical component of strategies to end the highly gendered global tuberculosis (TB) epidemic. Gender-responsive approaches that address cultural, structural, social, and individual determinants are essential to accelerate progress toward global targets to reduce TB morbidity and mortality.
The Gender Equity in TB working group was established in 2022 to mobilise knowledge on the role of gender in TB for awareness and action in TB prevention and care through evidence-informed policy and practice.
The objectives of this working group are:
• To establish an inclusive community of stakeholders including researchers, practitioners, policy makers, civil society, TB-affected communities and their coalitions
• To create an online network for working group members to share evidence on gender in TB burden, prevention, and care and guidelines and strategies for addressing gender disparities and improving gender equity in TB prevention and care
• To identify evidence and policy gaps, outline research priorities, and provide recommendations for change towards a gender-transformative response to TB
The working group has advocated for recognition of gender as a social determinant of TB ahead of the United Nations High Level Meeting on Tuberculosis and contributed to the Stop TB Partnership’s “The Accountability Report of TB-affected Communities & Civil Society: Priorities to Close the Deadly Divide”. The group has also hosted a series of symposia and webinars:
• “Enabling gender equity in TB: gender-sensitive solutions in TB policy and programme” at the Union World Conference on Lung Health
• “Multisectoral engagement to improve gender equity in TB and to ensure no one is left behind” on International Men’s Day 2022 co-hosted with the WHO Global TB Programme
• “Community, right and gender: Meaningful engagement with African-centred masculinities to end TB” co-hosted with The LIGHT Consortium and SSHIFTB
• “Raising the ambition for a gender-transformative response to tuberculosis for improving health, social and economic outcomes” at the 2023 Union World Conference on Lung Health
The group is currently co-chaired by:
Joseph Daniels (Arizona State University, USA)
and working closely with:
Katherine Horton (London School of Hygiene and Tropical Medicine, UK)
Kerry Millington (Liverpool School of Tropical Medicine, UK)
Amrita Daftary (York University, Canada)
Jeremiah Chikovore (Human Sciences Research Council, South Africa)
Joseph Daniels (Arizona State University, USA)
Maurine Murenga (TB Women Global, Kenya)
Andrew Medina-Marino (Desmond Tutu Health Foundation, South Africa)
and our group members.
Please contact us at genderequityintb@gmail.com
Working Group goal:
- To integrate effective tobacco control strategies into TB programs by fostering collaboration, building capacity, and promoting policy and practice changes that reduce the burden of smoking-related TB outcomes.
Objectives by Year
· By 2026: Revise and publish the updated edition of The Union’s Guide on Smoking Cessation and Smokefree Environments for people with TB ("Green Guide").
· By 2028: Facilitate the integration of smoking cessation interventions into national TB control programs in at least five countries.